On Nov. 15 a study compared adjunct therapy (niacin vs. ezitimibe) for patients with known coronary artery disease (CAD) and hypercholesterolemia. The results indicated that patients would be better of with niacin (results published elsewhere on this website).
The NYTimes commented on the study outcomes: Study Raises Questions About Cholesterol Drug’s Benefit on November 15, 2009: “For patients taking a statin to control high cholesterol, adding an old standby drug, niacin, was superior in reducing buildup in the carotid artery to adding Zetia, a newer drug that reduces bad cholesterol, according to a new study.” The next day, in a follow-up report: …”Merck investors viewed the results with relief, analysts said, because there was no sign that Zetia made the arterial condition worse.”
“The market worry was for a negative result,” Catherine J. Arnold, an analyst at Credit Suisse, wrote in a note sent to investors on Monday morning, “while the result was essentially no change for Zetia and positive results (plaque regression) for niacin.”
Merck’s stock closed at $33.81 a share, up 71 cents. Abbott’s closed at $53.63, up 68 cents.”
Zetia has been a polarizing drug among some doctors because, while it reduces bad cholesterol, it has not yet been proved to reduce the risk of heart problems — the ultimate purpose of a cholesterol medication.”
Now what does this mean?
If the data are correct, there appears a distinct advantage to the adjunct use of Niacin vs. Ezitimibe, with an effect that extends to improved HDL/LDL levels and decreased chance of adverse cardiovascular outcomes. However, is this a valid conclusion?
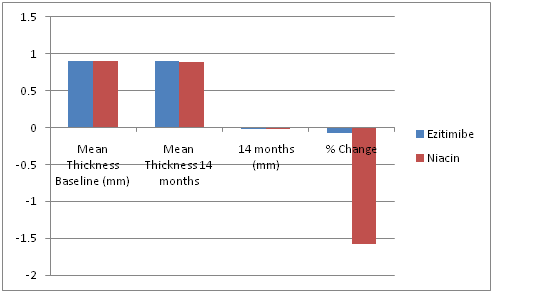
| Mean Thickness Baseline (mm) | Mean Thickness 14 months | 14 months (mm) | % Change | |
| Ezitimibe | 0.8957 | 0.895 | -0.0007 | -0.078151 |
| Niacin | 0.9001 | 0.8859 | -0.0142 | -1.577602 |
These findings generate a number of questions:
- The resolution of the Ultrasound linear-array probe (13 MHz Micromaxx, Sonosite) screen resolution is a pixel size of 0.082135 mm, or roughly 10% of the measurements that were taken. Is a 1.5% change in observations truly observable under those circumstances?
- While there is a statistically significant difference between the two drugs, a 1.5% improvement for Niacin, how much of that translates into something that is clinically usable?
In order for an atherosclerotic plaque (blockage) to become obstructive to blood flow, it is generally assumed that it has to involve >70% of the circumference of an artery. Successful treatment then is to reduce this obstruction by a minimum of 20%, since at 50% the obstruction is no longer flow limiting (not taking into account increased needs with exertion).
Using a reduction of 1.5% over a 14 months treatment period would result in >15 years of intense treatment with a drug (Niacin, vitamin B3) that is often poorly tolerated at high dosages (Flushing, itching, liver abnormalities).
Symptomatic patients or patients with tight lesions are at immediate risk, and don’t have time to wait for 14 months, let alone 15 years for reversal of their atherosclerosis. Studies like this point out the limitations of this type of treatment. However, they are quite useful as a treatment modality in patients with non-critical disease, or as adjunct therapy following an intervention such as PCI or CABG to prevent progression of disease elsewhere.
Dr T